
700 Glenhuntly Road
Caulfield VIC 3162
03 9044 4555

700 Glenhuntly Road
Caulfield VIC 3162
03 9044 4555
Periarticular Osteotomy for Knee Osteoarthritis
EXAMPLE ONLY
Osteoarthritis is a process of the gradual wearing out of the lining cartilage of the bones forming any joint in the body. In the knee, the lining cartilage covers the end of the femur (thigh bone), the top of the tibia (shin bone) and the undersurface of the patella (knee cap). When the cartilage wears, there is limited ability for it to heal itself and the worn cartilage is often associated with inflammation, pain and swelling of the affected joint.
The knee joint can be thought of as being composed of three compartments - the medial, lateral and patellofemoral compartments. Osteoarthritis may affect one, two or all three of these compartments to various degrees and the treatment for each may be slightly different. When all three compartments have advanced osteoarthritis that is painful, and all non-operative therapy has been exhausted, one appropriate surgical option may be a total knee replacement. However when the osteoarthritis is localised to one compartment and it is not advanced, an osteotomy might be more appropriate.
The aim of a periarticular osteotomy is to offload the compartment of the knee that is symptomatic. The goal is to reduce the painful symptoms of osteoarthritis when weight bearing occurs through the affected compartment. Another added effect is to potentially slow the progression of arthritis in this area. This is achieved by realigning the lower limb in such a way that when walking, weight is taken on the other unaffected part of the joint. For example, if the medial compartment of the knee joint is affected, then the aim is to realign the leg to allow weight to be shifted onto the unaffected lateral compartment.
By changing the alignment of the lower limb, this has the effect of changing the shape and outward appearance of the leg. For example, if an osteotomy is performed when there is initially a “bow-leg” shape to the lower limb, this usually results in a leg that becomes straight or even “knock-kneed”. The same is true for someone who is initially “knock-kneed”, that is, the result is for a straight or bowleg appearance.
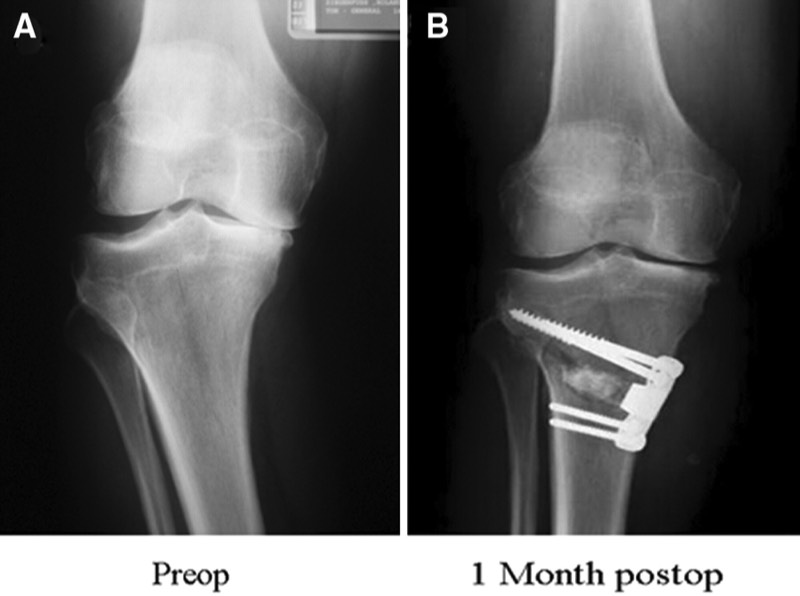
The osteotomy may be performed either on the femur or the tibia. If the leg is bowed to begin with, usually the osteotomy is performed on the tibia. If the leg is knock-kneed, then the osteotomy is usually performed on the femur. The former is the more common scenario, and usually the procedure involves realigning the leg by creating a cut in the bone and opening up a wedge shaped gap in the tibia. This is often referred to an opening wedge high tibial osteotomy (OW HTO). Alternatively, the other option for treating the same problem is to remove a small wedge of bone from the cut tibia. This is called a closing wedge high tibial osteotomy (CW HTO). Usually the osteotomy is held stable with a plate and screw type construct or with metallic staples. Both osteotomies have the same overall effect, however there are pros and cons with both. Ultimately, the decision as to which is best is decided on a patient-patient basis after consultation with the surgeon.
The procedure is usually performed under a general anaesthetic, and the inpatient stay can be up to two to three nights. Depending on the surgeon’s preferences, you may have a brace for a period of time postoperatively and you may be non or partial weight bearing with crutches for a period of 6 weeks while the bone heals.
The knee joint can be thought of as being composed of three compartments - the medial, lateral and patellofemoral compartments. Osteoarthritis may affect one, two or all three of these compartments to various degrees and the treatment for each may be slightly different. When all three compartments have advanced osteoarthritis that is painful, and all non-operative therapy has been exhausted, one appropriate surgical option may be a total knee replacement. However when the osteoarthritis is localised to one compartment and it is not advanced, an osteotomy might be more appropriate.
The aim of a periarticular osteotomy is to offload the compartment of the knee that is symptomatic. The goal is to reduce the painful symptoms of osteoarthritis when weight bearing occurs through the affected compartment. Another added effect is to potentially slow the progression of arthritis in this area. This is achieved by realigning the lower limb in such a way that when walking, weight is taken on the other unaffected part of the joint. For example, if the medial compartment of the knee joint is affected, then the aim is to realign the leg to allow weight to be shifted onto the unaffected lateral compartment.
By changing the alignment of the lower limb, this has the effect of changing the shape and outward appearance of the leg. For example, if an osteotomy is performed when there is initially a “bow-leg” shape to the lower limb, this usually results in a leg that becomes straight or even “knock-kneed”. The same is true for someone who is initially “knock-kneed”, that is, the result is for a straight or bowleg appearance.
The osteotomy may be performed either on the femur or the tibia. If the leg is bowed to begin with, usually the osteotomy is performed on the tibia. If the leg is knock-kneed, then the osteotomy is usually performed on the femur. The former is the more common scenario, and usually the procedure involves realigning the leg by creating a cut in the bone and opening up a wedge shaped gap in the tibia. This is often referred to an opening wedge high tibial osteotomy (OW HTO). Alternatively, the other option for treating the same problem is to remove a small wedge of bone from the cut tibia. This is called a closing wedge high tibial osteotomy (CW HTO). Usually the osteotomy is held stable with a plate and screw type construct or with metallic staples. Both osteotomies have the same overall effect, however there are pros and cons with both. Ultimately, the decision as to which is best is decided on a patient-patient basis after consultation with the surgeon.
The procedure is usually performed under a general anaesthetic, and the inpatient stay can be up to two to three nights. Depending on the surgeon’s preferences, you may have a brace for a period of time postoperatively and you may be non or partial weight bearing with crutches for a period of 6 weeks while the bone heals.
Potential Complications
No surgery is without the potential for complications. These can be classified as general complications and those specific to this operation.
General complications
These complications relate to all types of orthopaedic surgery and include those related to the anaesthetic, wound site infection, bleeding and damage to nerves and blood vessels. Lower limb orthopaedic surgery also carries the risk of deep venous thrombosis and pulmonary embolism (DVT and PE). Please refer to the General Orthopaedic Surgical Complications information sheet for further details of these complications.
Specific Complications for Periarticular Osteotomy
Delayed Union and Non Union
This refers to slow (or no) bone healing at the osteotomy site. This may occur because the bone has been cut and needs time to heal. Delayed healing may be due to a number of causes and all of these are addressed should this issue arise. More surgery may be required to encourage to bone to heal faster in some settings.
Fracture
Once again, as the bone is being cut, there is the potential for fracture to occur into the joint or below the joint level. This is usually dealt with at the time of surgery if it occurs.
Ongoing Pain
If pain persists following an osteotomy this may be due to many different causes which is best assessed by the treating surgeon. Potential reasons include progression of arthritis to other compartments within the knee and pain related to prominent metal ware used to stabilise the osteotomy. The fixation device may be able to be removed at a later date once the osteotomy has healed and full function has been regained. This is an individual decision and different surgeons have different opinions regarding metal ware removal and the timing for this. This is best discussed with the surgeon individually.
The information above is general. All surgical procedures involve some risk. If you would like advice on your specific condition, please contact Oasis Orthopaedics to make an appointment with one of our specialists.