
700 Glenhuntly Road
Caulfield VIC 3162
03 9044 4555

700 Glenhuntly Road
Caulfield VIC 3162
03 9044 4555

Trauma and Fractures
What is a fracture?
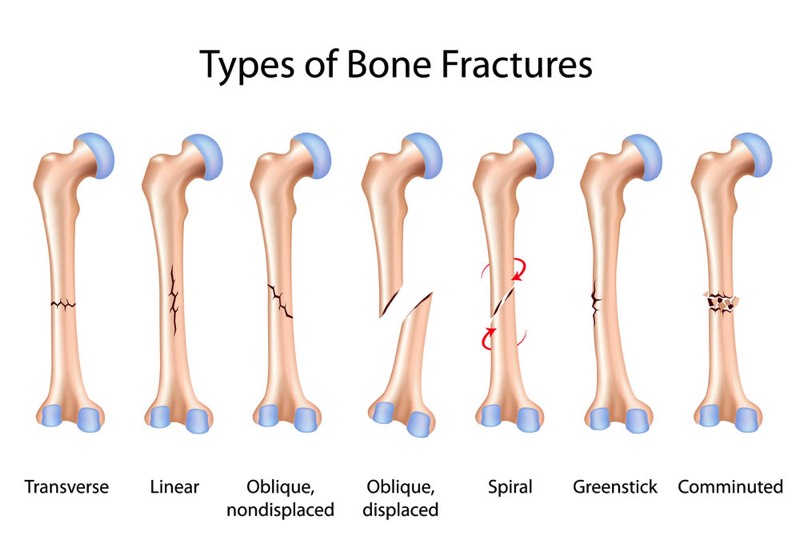
A fracture is ANY break or loss of continuity in the structure of a bone, whether it is a tiny crack all the way up to a bone that has split into multiple fragments.
Fractured bones may be undisplaced (a tiny crack in the bone without any significant separation of the fragments) or displaced (where there is a detectable separation of the bone ends).
Different types of fractures
In normal bones, fractures usually occur when a sudden amount of high force is applied to the bone. A “pathological fracture” is a fracture that occurs in a bone with abnormally reduced strength that experiences otherwise normal forces. There are a number of different causes of bone weakness, including osteoporosis, genetic abnormalities in bone formation and maintenance, developmental abnormalities of bone, non-cancerous and cancerous tumours, and infections.
Stress fractures occur in normal bones, but these bones are exposed to excessive/repeated loading and unloading, above what would be considered normal everyday activites. They are frequently seen in the lower limbs of athletes who run or jump, or soldiers who march long distances with heavy packs (e.g. stress fractures in the metatarsals of the feet or in the lower end of the tibia).
How can it be treated?
Most fractures tend to mend best if the surfaces of the broken bone are very near each other and the fine tissue lining the bone (periosteum) is relatively intact. When the bone breaks, the bone marrow bleeds and forms a clot (over a few hours) which is gradually converted by cells in the periosteum into fibrous scar tissue initially (over a few weeks) and this is later converted into calcified tissue (a few weeks or months later) – i.e. a basic form of bone again. With time this basic bone is then matured into more normal bone over a few more months. This is a biological process which is unable to be accelerated, generally, however, in some instances the healing process can be slowed down beyond what is normally seen. In particular, smoking tobacco in any form will essentially hinder the cells responsible for converting the blood clot into calcified tissue and will reduce the rate of healing of a fracture. In many cases, smoking may stop healing altogether. When bone does not heal in a timely manner for what is expected it is called a “non-union”. Those with diabetes are also known to have a reduced rate of healing fractures. Some bones are also known to have a poor blood supply and may be more prone to non-union. These include the scaphoid bone in the wrist, the neck of the talus in the ankle and the shaft of the tibia. If the fragments of bone that has a normal healing potential are separated by a long distance (which usually means significant damage to the healing periosteum), they may also fail to heal.
For healing of bone (union) to occur, not only must the ends of the bone be nearby, but the fragments usually need to be immobilised for sufficient time for the healing process to get under way. This also depends on the location of the fracture and the age of the patient. In general children tend to heal more rapidly than adults and upper limb injuries tend to unite more quickly than lower limb injuries. Again, this depends somewhat on which bone (and sometimes which part of the bone) is fractured.
The methods of treatment of fractures can take many forms, but can broadly be grouped into “closed” and “open” methods. Closed methods utilise techniques where the broken bone itself is not directly manipulated, but is done so indirectly by applying gentle but firm pressure on the bone with the skin and muscles left intact – i.e. no incisions are made and the bone is not “seen” by the surgeon. These include the use of external immobilisation of the broken bone by use of a splint or brace, a circumferential plaster cast or an external fixateur. Open methods involve the surgeon making an incision in the skin and splitting muscles to allow direct manipulation of the broken bone ends so that they are accurately placed as close as possible to their original position. Open techniques include internal fixation with plates and screws on the external surface of a bone, and with intramedullary rods which are implanted within the bone marrow of the bone.
Closed Treatment of Fractures
The simplest method is to use an external splint or functional brace, which may be worn under or over clothing to hold the limb/broken bone still. This has the advantage of being removable, not overly constrictive, and its position may be adjusted if there is swelling. As there is no incision made in the skin, there is no risk of infection, bleeding or nerve and blood vessel injury. However, this is also a disadvantage as the fractured bone may be permitted excessive mobility and then may fail to unite.
A cylindrical/circumferential cast is more conforming and restrictive than a splint. This is made out of Plaster of Paris or synthetic material such as fibreglass or casting tape. This cast encloses a portion of the broken limb and has the advantage of being highly conforming and thus very good at immobilising the fracture, as long as there is minimal swelling. It also does not run the risks of surgery such as infection, bleeding or nerve and blood vessel injury.
Closed management of fractures does not always allow precise placement of bone fragments if they have been significantly displaced, unless an anaesthetic is administered to permit the surgeon to manipulate of the fracture fragments (without making any skin incisions). This is called a “closed reduction” or a GAMP (General Anaesthetic, Manipulation and Plaster).
If the fragments of bone are too unstable or to large to be managed in an external splint or plaster (e.g. a fractured femur), one option may be to use multiple rigid pins which pass from outside the skin into the broken bones, and then to connect these pins to larger rods to form an external frame, linked to the bone. This is called “external fixation”, and has the advantage of having a solid, direct grip on the bone fragments but without disturbing the soft tissues around the bone and allowing the fracture to be reasonably well immobilised. The disadvantages of this technique include infection by the patients skin germs tracking down the external surface of the pins, the pins may loosen from the bone, the fixation may not be strong enough to permit immediate or early weight bearing or range of movement, and there is a small chance of nerve or blood vessel injury. The pins also need to be removed eventually, usually requiring a further anaesthetic to do this.
Open Treatment of Fractures
If the fracture fragments are more significantly displaced, or involve the surface of an important joint then open methods of fracture management may be required. The surgeon will perform an “open reduction”, where an incision is made in the skin, the muscles and other vital structures like nerves and arteries are moved to allow visualisation of the broken ends of the bone to bring them closer together with less deformity. With fractures that are significantly displaced and risk progression to a non-union, this technique is used to bring the bone ends close enough enable the fragments to heal, and has the advantages of permitting healing with much less deformity, earlier movement of the joints on either side of the broken bone or earlier bearing of weight.
Open reduction and internal fixation (ORIF) of fractures will not necessarily increase the speed at which the fracture heals, but makes healing more certain and should reduce the amount of deformity/disability encountered if the same injury were to be treated by closed means.
Fractures that involve the cartilage surfaces of important joints such as the wrist, elbow, shoulder, hip, knee and ankle usually have a higher probability of developing post traumatic arthritis (pain and stiffness) if the fragments of bone have greater than 2mm of separation at the surface of the joint.
ORIF has the disadvantages of infection, bleeding, nerve and vessel injury and occasionally may require secondary surgery to remove implants once the fracture has healed if they cause irritation of nearby structures or prominence under the skin. Fortunately, these problems are not common.
Dislocations and Severe Soft Tissue Injuries
A dislocation is an injury where parts of a joint are completely separated and can no longer move in their normal fashion. The more commonly dislocated joints include:
- The shoulder (gleno-humeral) joint
- The acromio-clavicular joint (AC joint or collarbone)
- The kneecap (patello-femoral) joint
- The small joints of the fingers (interphalangeal joints).
These are fairly common injuries and can frequently be treated by manipulating the dislocated joint back into normal alignment initially, also called a “closed reduction”. Any other joint in the body can dislocate, although they tend to be less common.
There are a few structural features of any joint that help keep all the components moving together and preventing most peoples’ joint from dislocating. These include:
- the conforming shapes of the two bones involved in forming the joint;
- the ligaments that hold the bones in the joint together;
- and the strength and direction of force of the muscles that move the joint.
In general terms, there will be an abnormality of one or more of these structural components that will lead a joint to dislocate. Moreover, once a joint has dislocated there is often irreversible damage to either the muscles or ligaments that normally control the joint and this makes repeated dislocations much more likely. This is especially the case in the shoulder and patella, and also in the case of young children or adolescents, resulting in recurrent instability of the joint, more so than adults. While recurrent instability of a joint itself may be disabling, there will often be associated damage to the cartilage surfaces that can occur with the initial or subsequent dislocations and this may lead to later arthritis.
Very rarely it may be impossible to reduce the dislocation with closed techniques as muscle, tendon or nerves may have been trapped between the joint surfaces. In these uncommon cases an operation will be required to perform an “open reduction”, which allows the surgeon to remove the interposing structure and return the bones to their correct position.
The information above is general. All surgical procedures involve some risk. If you would like advice on your specific condition, please contact Oasis Orthopaedics to make an appointment with one of our specialists.